This method helps reduce postoperative nausea and vomiting, causes less laryngeal trauma, and avoids complications associated with endotracheal intubation. Anesthetic agents are delivered and maintained through a specialized device called a laryngeal mask airway.
This technique is suitable for minimally invasive, low-trauma, short-duration procedures and does not require muscle relaxants. This crucial omission reduces complications such as postoperative respiratory depression due to residual muscle relaxants, allergic or anaphylactic reactions, and the risk of prolonged muscle weakness—particularly in elderly patients or those with neuromuscular conditions.
|
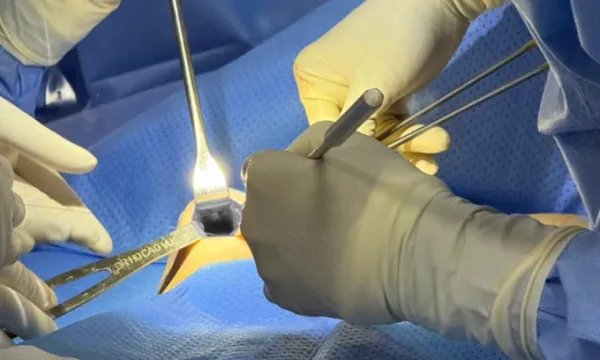
Adjusting the gap between the first ring and the other ring using laryngeal mask anesthesia. Photos courtesy of Dr. Cao Vu –> Cần thay ảnh dùng text TV |
MD, MSc. Ho Cao Vu shared that for many years he used endotracheal intubation anesthesia in breast implant explantation or, in some cases, local anesthesia combined with sedation.
However, observing the disadvantages of these methods, he has since transitioned to using laryngeal mask anesthesia in 100% of breast implant explantation and replacement surgeries that do not involve complex abnormalities or prolonged operating time (with the exception of grade 4 capsular contracture cases).
For the anesthesia team at the general hospital to agree to transition from endotracheal intubation to laryngeal mask anesthesia in breast implant explantation and replacement, the surgeon must ensure rapid surgery, minimal tissue trauma, minimal invasiveness, and limited manipulation of the pectoralis muscle (as laryngeal mask anesthesia typically does not use muscle relaxants).
 |
|
After assessing the current situation, Dr. Vu used an ultrasound scalpel to revise the pocket to fit the new breast implant. Photo courtesy of Dr. Cao Vu |
Dr. Vu applies ultrasonic point dissection as a standard technique, which allows standard breast implant explantation procedures to take only 15–30 minutes (from skin incision to wound closure). Surgeries requiring pocket revision and implant replacement typically take 30–60 minutes, with minimal trauma, no bleeding, no seroma, no drains, and no need for postoperative analgesics or antibiotics. For these reasons, his standard breast implant explantation and replacement procedures are now performed under laryngeal mask anesthesia.
The advantage of not using muscle relaxants in laryngeal mask anesthesia for breast implant explantation or explantation with new implant placement is that it allows the surgeon to reassess the current implant pocket, pocket pressure (excess or deficiency), and the condition of the pectoralis muscle, including muscle position, degree of contraction or relaxation, and the level of fibrosis (firm or soft).
|
Implant pocket dissection. Photo courtesy of Dr. Ho Cao Vu |
Below is a sharing from Dr. Vu, who has performed more than 200 breast implant explantation and replacement procedures, regarding the advantages of laryngeal mask anesthesia during ultrasonic point dissection with the new-generation ultrasonic scalpel.
1. Accurate assessment of pocket pressure
The surgeon explains that the most common implant placement planes today are submuscular or dual-plane. For this reason, the pectoralis muscle plays an essential role in determining breast shape, pocket pressure, implant longevity, and, in some cases, the overall softness of the breast.
Each patient has different anatomical characteristics, including variations in the pectoralis muscle. In patients with previous implants, the implant pocket has already formed around the implant. The surgeon enters the pocket and evaluates pocket pressure, areas of pocket excess or deficiency to allow the implant to lie evenly, the degree of muscle fibrosis, the condition of the previous implant (folding, rupture, brand, diameter, projection), and chest wall morphology (pectus carinatum or pectus excavatum).
Based on the current condition and the patient’s expectations, Dr. Vu uses the ultrasonic scalpel to revise the implant pocket to accommodate the new implant (upsizing, downsizing, maintaining the same size, increasing projection, or reducing projection).
With endotracheal anesthesia using muscle relaxants, the surgeon cannot accurately assess baseline muscle tone, as the pectoralis muscle returns to its physiologic state only after emergence. For this reason, laryngeal mask anesthesia allows the surgeon to evaluate pocket pressure precisely and perform accurate implant pocket revision, reducing late complications such as muscle tightening that causes implant folding, compression on the implant, shortened implant lifespan causing early implant rupture, and increased capsular contracture rates.
2. Rapid pocket dissection and revision
Prolonged operating time can affect patient comfort, especially in older patients who previously experienced painful breast augmentation and are fearful of undergoing implant removal. Understanding these concerns and expectations, Dr. Vu continually refines his dissection technique to optimize surgical time.
The use of laryngeal mask anesthesia in breast implant explantation, combined with ultrasonic point dissection, reduces the explantation procedure to only 15–30 minutes.
Cases requiring dissection and precise revision of pocket pressure can be performed accurately without muscle relaxants. Patients recover quickly, are discharged within 4–6 hours, and do not require postoperative analgesics or antibiotics. Many patients in their 50s and 60s have chosen this method because it ensures excellent safety.







