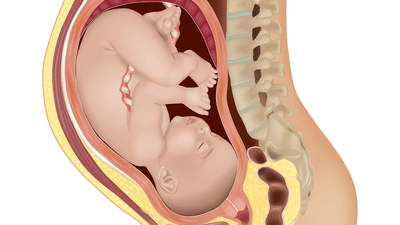
When your baby begins their journey through the birth canal, their head has to navigate the curve of your pelvis like a key fitting through a lock. For most births, the baby’s head flexes and rotates smoothly so that it fits the pelvic opening at just the right angle. But sometimes, the head leans to one side instead of staying straight; this sideways tilt is called
asynclitism.
In many labours, asynclitism corrects itself as contractions continue and the baby shifts naturally. Yet in others, the tilt can make progress slower, increase the need for repositioning or intervention, and sometimes add to maternal exhaustion. Understanding what it means helps you work with your care team instead of worrying that your body isn’t doing what it should.
What Asynclitism Actually Means
Asynclitism describes the way your baby’s head sits in the pelvis when it’s not aligned perfectly in the centre. Imagine the baby’s head tilting slightly, so that one parietal bone (side of the skull) is closer to the cervix than the other.
There are two main types:
- Anterior asynclitism: The baby’s head tilts so the front side of the head (toward the face) leads through the pelvis.
- Posterior asynclitism: The back of the head (occiput) tilts forward, making the posterior side lead.
Both can occur naturally as the baby tries to find the easiest way down the birth canal. During a vaginal examination, your doctor or midwife may feel one of the baby’s parietal bones more prominently. In some hospitals, ultrasound is also used to confirm this position, especially if labour progress slows or descent seems uneven.
Mild asynclitism is very common and often part of a healthy, adaptive labour process. It only becomes a concern when the tilt is severe enough to stop descent or when contractions fail to move the baby into alignment.
Why It Matters for Labour Progress
When the head enters the pelvis at an angle, it may not apply even pressure on the cervix. This can lead to:
- Slow dilation: The cervix may open unevenly because pressure isn’t centred.
- Prolonged or irregular contractions: The uterus works harder to rotate and reposition the baby.
- Pelvic pain or backache: The uneven pressure can cause discomfort in the lower back or hips.
- Increased chance of assisted delivery: Severe or persistent asynclitism may require vacuum, forceps, or, rarely, a caesarean section.
However, a tilted head does not mean labour will necessarily end in surgery. Many babies naturally correct their position during contractions or as you change posture. Your body’s movements, walking, kneeling, or squatting, can help the head adjust and align more symmetrically.
What Causes the Head Tilt?
Asynclitism can occur for several reasons, most of them simple mechanical or positional factors rather than medical issues:
- Pelvic shape and space: Every pelvis has a slightly different shape. A narrow or asymmetric pelvic inlet can make the baby’s head enter at an angle.
- Uterine tone and contractions: Strong, uneven contractions can push the baby’s head off-centre early in labour.
- Baby’s position: Babies in occiput posterior (facing the mother’s abdomen) positions often enter the pelvis with a tilt before rotating forward.
- Epidural anaesthesia: While pain relief is safe and effective, limited movement after an epidural can make it harder for the baby to rotate freely.
- Tight pelvic floor muscles: A strong or tense pelvic floor may guide the baby’s head unevenly.
- Lying flat for long periods: Staying on your back for hours can restrict pelvic mobility and slow rotation.
In most cases, asynclitism is a combination of these factors, not something caused by your choices or body “failing.” It reflects how dynamic and adaptive labour really is.
How Doctors Identify It
Your obstetrician or midwife may suspect asynclitism if:
- Labour progress slows despite good contractions.
- The baby’s head doesn’t descend as expected on vaginal examination.
- The cervix feels unevenly pressed, or the presenting part isn’t centred.
Clinical assessment: During a vaginal exam, the provider may feel one side of the skull higher than the other, or the sagittal suture (the midline of the skull) closer to the front or back of the pelvis.
Ultrasound confirmation: Modern intrapartum ultrasound can show the baby’s head angle and position in real time, helping distinguish asynclitism from other causes of obstructed labour like malpresentation or cephalopelvic disproportion (CPD).
Differentiation from CPD: Unlike CPD, where the pelvis is too small for the baby’s size, asynclitism is usually positional and can be corrected with posture, movement, or time.
How It’s Managed?
Management depends on how much the head is tilted and how well the labour is progressing. The goal is to help the baby rotate and align naturally before resorting to medical intervention.
1. Maternal repositioning and movement
- Changing your position frequently can help open the pelvis and encourage rotation.
- Useful positions include:
- Hands and knees: Relieves back pressure and allows gravity to help reposition the baby.
- Side-lying (opposite the baby’s back): Encourages rotation toward the correct angle.
- Lunging or using a birth ball: Increases pelvic space and flexibility.
- Squatting or upright positions: Allows gravity to assist descent once alignment improves.
2. Avoiding prolonged lying on the back
Staying supine restricts pelvic mobility and may worsen asynclitism. Even small shifts, like leaning on one side with a pillow, can help.
3. Monitoring and patience
Mild cases often correct themselves with contractions. As long as your baby’s heart rate is normal and progress continues, doctors usually allow time for natural adjustment.
4. Assisted delivery or caesarean section
If labour stalls or the baby shows distress, your obstetrician may use instruments such as a vacuum or forceps to help rotate and guide the head. In rare cases where descent remains blocked, a caesarean birth may be the safest option.
5. Supportive care
Pain relief, hydration, and emotional reassurance play vital roles. Long labours caused by asynclitism can be exhausting, and rest periods between contractions can make a big difference in preserving strength for pushing.
Emotional and Physical Support
Prolonged labour can test your patience and endurance. You may feel frustrated, anxious, or even guilty, as if something is “wrong” with you. It’s important to remember that asynclitism is not your fault, nor is it a reflection of how well your body can birth.
How to cope and stay supported:
- Ask your birth team to explain what’s happening clearly; understanding often reduces fear.
- Use breathing, guided relaxation, or massage to ease tension in your pelvis and lower back.
- If you have a partner, encourage gentle back pressure or hip squeezes during contractions.
- Request position changes even if you have an epidural; your midwife can help shift you safely.
- Focus on progress, not time. Every contraction still brings your baby closer, even if dilation feels slow.
Emotional support during a long labour isn’t just comforting; it helps regulate stress hormones that can actually influence oxytocin release and contraction strength. Staying calm, hydrated, and reassured gives your body the best chance to correct the tilt naturally.
Asynclitism is one of the body’s many ways of negotiating space during labour. While it can make progress slower or more uncomfortable, it’s rarely dangerous when monitored carefully. Most babies correct their position on their own, and with guidance, movement, and support, your labour can still unfold safely and naturally. Understanding this small tilt can turn confusion into confidence, a reminder that every birth follows its own rhythm, and yours is no exception.
Whether you’re pregnant, a new mom, or navigating postpartum, you don’t have to do it alone. Join our support group
to connect, share, and support one another.
FAQs on Asynclitism: When the Baby’s Head Tilts Slightly and Slows Labour
Can asynclitism correct itself during labour?
Yes. In most cases, the baby’s head gradually realigns as contractions and maternal movements help reposition it. Many women go on to have normal vaginal deliveries.
Does it mean my pelvis is too small?
Not necessarily. Asynclitism usually reflects temporary positioning rather than pelvic size. Only in rare cases of true cephalopelvic disproportion would size be a limiting factor.
Can I still have a vaginal birth?
Yes, especially if your baby’s heart rate remains normal and contractions are effective. Your care team may use position changes, patience, or assisted delivery methods to help.